NHS dermatology access gap: where it's straining and what can help





A clinician reviewing a case on the Legit.Health interface.
Skin disease accounts for around 24% of consultations with general practitioners (GPs) in the United Kingdom. 1 Across England alone, that translates to roughly 13 million skin-related primary-care attendances every year. 2 On any given week, a meaningful share of every GP's caseload involves a rash, a lesion, an itch, a flare or a follow-up question about a long-running condition such as eczema, psoriasis, acne or hidradenitis suppurativa.
Skin cancer dominates the conversation about dermatology because it is urgent and time-sensitive. But it is not what most patients walk in with. Across published UK and international studies, malignant skin conditions account for only around 5% of the dermatology cases seen in primary care; the other 95% are inflammatory, infectious, autoimmune or follow-up presentations. See our analysis of dermatology case-mix. The pathway has to work for both ends of that spectrum, not just the urgent slice.
Diagnosis support across the spectrum, from suspected skin cancer to a common bacterial infection, looks like this:
- Cutaneous melanoma47.7%
- Basal cell carcinoma1.24%
- Intraepidermal squamous cell carcinoma0.41%
- Lymphatic malformation0.36%
- Plane warts0.36%
- Cutaneous melanoma
- Basal cell carcinoma
- Intraepidermal squamous cell carcinoma
- Lymphatic malformation
- Plane warts
- Other

- Impetigo77.53%
- Cutaneous leishmaniasis1.95%
- Bullous impetigo1.03%
- Furuncle0.59%
- Tinea faciei0.48%
- Impetigo
- Cutaneous leishmaniasis
- Bullous impetigo
- Furuncle
- Tinea faciei
- Other

The mix matters. Suspected skin cancer is the most urgent slice of dermatology, but it is far from the largest. The bulk of what GPs see is chronic, inflammatory or infectious skin disease, and most of those cases never need a hospital outpatient slot.
Yet for many of those patients, the next step in the pathway is a long wait. NHS England's Referral to Treatment (RTT) data place dermatology among the longest waiting specialties in the country. 3 In parts of England, the median wait for a first dermatology appointment is 17 weeks, and people referred urgently on the suspected-skin-cancer 2-week-wait (2WW) pathway sit in one of the largest 2WW cohorts in the system. 4
The shape of the problem is not a single bottleneck. It is a structural mismatch between rising demand and a finite specialist workforce, made worse by a primary-to-secondary handover that was not designed for the volume or the visual nature of dermatology.
A specialty that is everywhere in primary care, and concentrated everywhere else
The first thing to notice about UK dermatology is that almost all of the patient-facing work happens in primary care. Skin is consistently among the top reasons for new GP consultations. 1 5 Most of those consultations are managed and resolved entirely by the GP. Some practices have a dermatoscope on hand, and some GPs hold extended training in dermatology through bodies such as the Primary Care Dermatology Society — but provision is uneven, and where you sit on the GP rota still functions as a postcode lottery for whether the patient meets a clinician with that extra training. Even where it exists, primary-care dermatoscopy and GPwER coverage is a partial answer rather than a substitute for specialist input — and that is precisely the gap an AI-supported workflow can help close.
When a GP does need specialist support, the route to it is narrow. The British Association of Dermatologists has documented for years that the consultant dermatology workforce is finite and unevenly distributed across the four nations. 6 The Getting It Right First Time (GIRFT) programme described the same thing in its 2021 specialty report: significant regional variation, vacancy rates, and a service that struggles to absorb routine and urgent demand at the same time. 7
- Skin disease drives ~24% of UK GP consultations, yet NHS dermatology RTT waits are among the longest of any specialty.
- The pathway breaks at the front door, the referral gate, and in chronic-disease follow-up.
- Legit.Health is a CE-marked, MHRA-registered AI medical device that lives inside the EHR and supports the full dermatology spectrum.
The numbers add up to a system where the bottleneck is not in any one place. It is at the front door, at the referral gate, and at follow-up.
Where the pathway breaks
There are three failure points worth naming.
At first contact. A GP is asked to decide what is urgent without specialist eyes. Photo quality varies clinic to clinic, severity descriptions are written in free text, and the referral letter is the only structured object that travels onward. Two GPs looking at the same lesion can write very different referrals.
At the referral gate. RTT dermatology waits sit among the longest of any specialty. 3 Suspected skin cancer travels via the 2WW pathway, and the volume on that pathway has grown faster than the capacity to absorb it. 4 Benign and high-risk cases queue together. Triage is mostly text-based, downstream of the imaging that should have informed it.
In follow-up. Chronic skin disease, the kind a GP sees week after week, is rated by impression rather than measurement. Severity scores such as the Psoriasis Area and Severity Index (PASI) and the SCORing Atopic Dermatitis (SCORAD) index exist precisely so that "is this getting better" can be answered with data; in everyday practice, they are calculated by hand if at all. The result is a follow-up loop where change over time is hard to capture reproducibly.
Möchten Sie die klinische KI-Technologie in Aktion sehen?
What would "good" look like?
A more workable dermatology pathway needs these ingredients:
- Standardised image capture at the moment of consultation, every time, regardless of who is holding the phone.
- Image quality assessment — automated checks that the photograph is dermatologically usable before it ever leaves the GP's screen, so that downstream decisions are not made on a blurred or poorly lit image. We have published peer-reviewed work on exactly this problem; see our Dermatology Image Quality Assessment (DIQA) study for the methodology and results.
- Diagnosis support at the front door — a structured read of the conditions a lesion or rash is most likely to be, alongside the clinician's own judgement, before any referral letter is written.
- Triage prioritisation so that a possible skin cancer is flagged for urgent review within hours, while a mild acne case is scheduled into a more appropriate slot. The 2WW pathway works only if the cases reaching it are the ones that truly need it.
- Objective severity measurement for the chronic conditions where follow-up matters most (psoriasis, eczema, acne, hidradenitis suppurativa, urticaria, alopecia).
- Structured referral data that travels with the patient, so that the specialist receives the same shape of information from every clinic.
- Longitudinal monitoring that lets clinician and patient see whether the treatment is working without having to remember what the lesion looked like three months ago.
What changes the picture in 2026 is that all of this can be delivered inside a routine GP consultation, in seconds, on hardware the practice already owns — without asking the clinic to redesign how it works.
Where AI-supported workflows fit
This is the gap an AI-supported dermatology workflow is designed to close. A regulated medical device that lives inside the consultation, trained to recognise dermatological presentations and to compute severity scores from a clinical image, can do three things at once: it can standardise capture, return an objective assessment, and structure the data that gets sent onwards.
Legit.Health is one such platform. It is a CE-marked, MHRA-registered medical device built to support the full dermatology spectrum: structured triage at first contact, objective severity scoring for chronic disease, and reproducible follow-up over time. The clinician keeps clinical judgement. The platform brings the data.
In practice, the workflow inside the clinician's electronic health record runs in three steps: select the body area, upload and analyse the image, and read the ranked output.
1. Body area
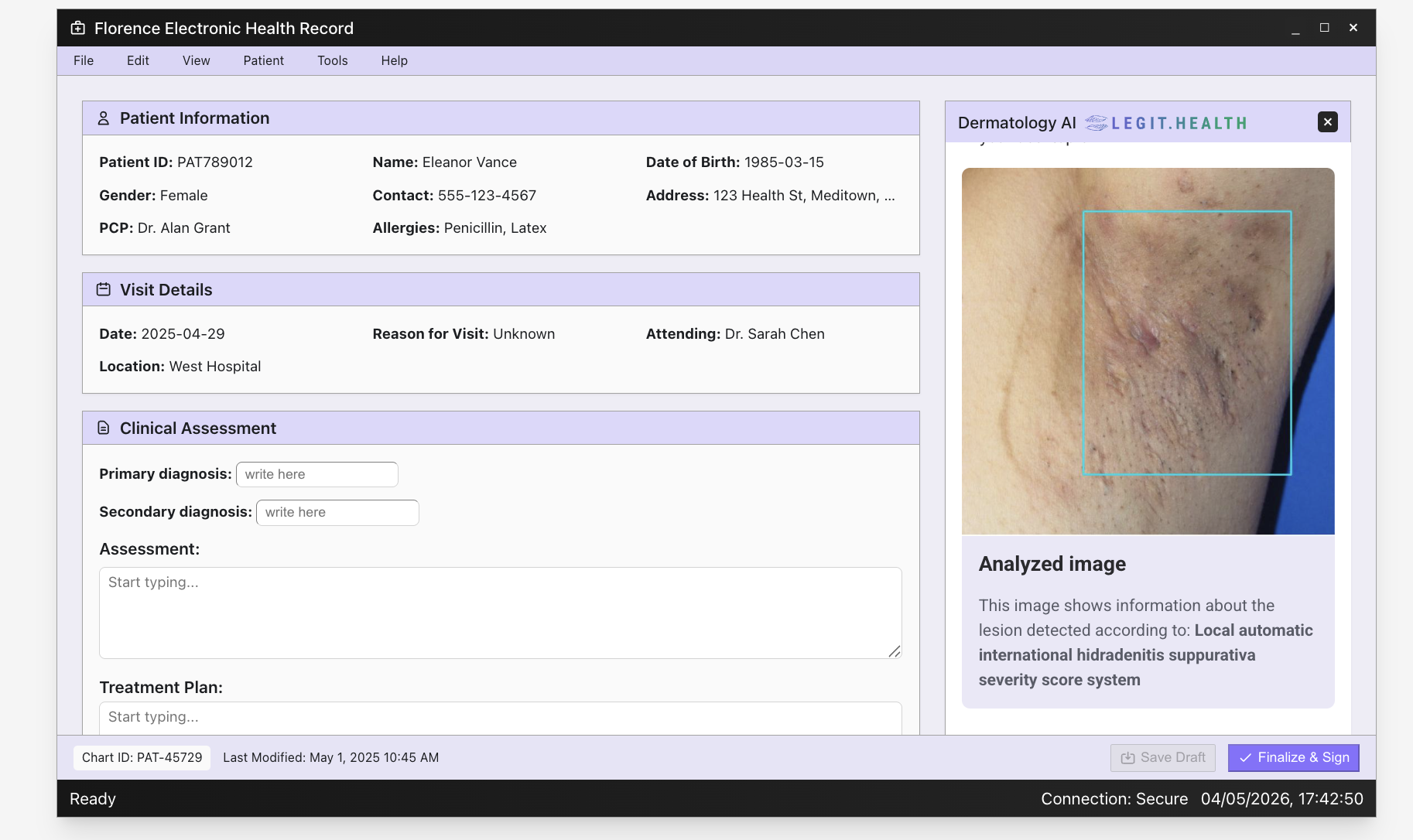
2. Image analysis
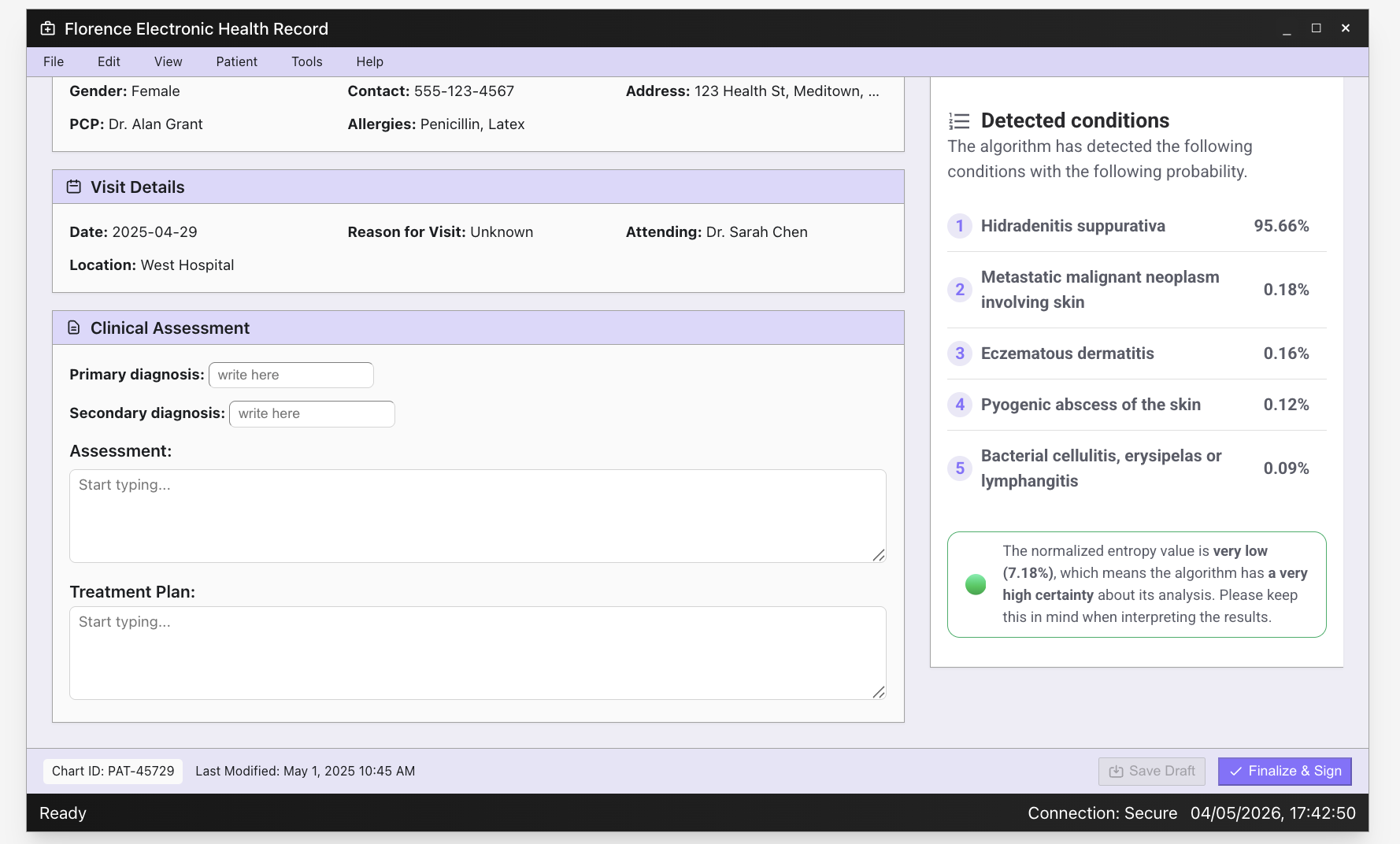
3. Top-5 detected conditions
The same diagnosis-support engine runs across chronic inflammatory disease and autoimmune presentations:
- Generalised pustular psoriasis77.03%
- Pustular psoriasis2.31%
- Pemphigus0.95%
- Zoster0.48%
- Cutaneous tuberculosis0.48%
- Generalised pustular psoriasis
- Pustular psoriasis
- Pemphigus
- Zoster
- Cutaneous tuberculosis
- Other

- Cutaneous lupus erythematosus50.11%
- Necrobiosis lipoidica1.42%
- Dermatosis neglecta1.26%
- Cutaneous tuberculosis1.14%
- Benign familial pemphigus1.03%
- Cutaneous lupus erythematosus
- Necrobiosis lipoidica
- Dermatosis neglecta
- Cutaneous tuberculosis
- Benign familial pemphigus
- Other

That breadth is what makes the device fit a primary-care consultation, where the clinician does not know in advance what is about to walk through the door.
In deployments, AI-supported triage and severity scoring have been associated with up to a 33% reduction in unnecessary specialist referrals, and with 82% of primary-care clinicians reporting greater diagnostic confidence after introducing the tool into their consultation flow. 8 The same body of evidence has shown an increase in the share of skin conditions resolved in primary care, freeing specialist clinics for the cases that genuinely need them.
These are early signals from operator and provider deployments, not silver bullets. What they suggest is more modest and more interesting: that giving primary care better data at the point of decision changes the shape of demand on the specialty, before any new consultant is hired.
Built for the NHS pathway
For an NHS or private UK provider, the practical questions are about regulation, integration and information governance.
Legit.Health is a regulated medical device with Conformité Européenne (CE) marking, registration with the Medicines and Healthcare products Regulatory Agency (MHRA), and certification under ISO 13485 (medical-device quality management) and ISO 27001 (information-security management). It integrates with the electronic health records (EHRs) that primary care already runs on, including EMIS, so that it sits inside the consultation rather than beside it. Patient data flows under the UK General Data Protection Regulation (UK GDPR) and the Data Protection Act 2018; the platform is designed to fit into existing information governance and clinical safety processes.
What the platform does not try to do is redesign the NHS dermatology pathway from scratch. The aim is the opposite: to slot into the GP appointment, the e-referral letter, the dermatologist's clinic and the patient's follow-up review without asking any of them to change how they work.
How this maps to the NHS 10-Year Plan
The NHS 10-Year Health Plan has been explicit about the direction of travel for the service. It names three strategic shifts: from hospital to community, from sickness to prevention, and from analogue to digital. Dermatology is one of the specialties where all three shifts meet, and where the gap between current state and stated direction is widest.
From hospital to community. Most skin disease is, and should be, managed in primary care. The 10-Year Plan's neighbourhood health model is built on the idea that more diagnostic and decision-support capability sits with the GP, the practice nurse and the community pharmacist. An AI-supported triage and severity tool gives those clinicians better data at the point of decision, so that fewer cases need to travel into hospital outpatient clinics in the first place.
From sickness to prevention. The 2WW pathway exists precisely because catching skin cancer early changes the outcome. A standardised image and a structured assessment at first contact make earlier detection more reliable. The same logic applies to chronic conditions: an objective severity score in primary care lets a clinician notice deterioration months before a hospital review would, and act on it.
From analogue to digital. The 10-Year Plan asks for digital tools that live inside the clinical workflow, not beside it. That means integration with the electronic health records (EHRs) that primary care already uses (EMIS being the largest), structured data that flows on with the referral, and devices that are regulated and information-governance-ready out of the box. A dermatology pathway that runs on free-text referrals and hand-calculated scores is, in 2026, the analogue half of that equation.
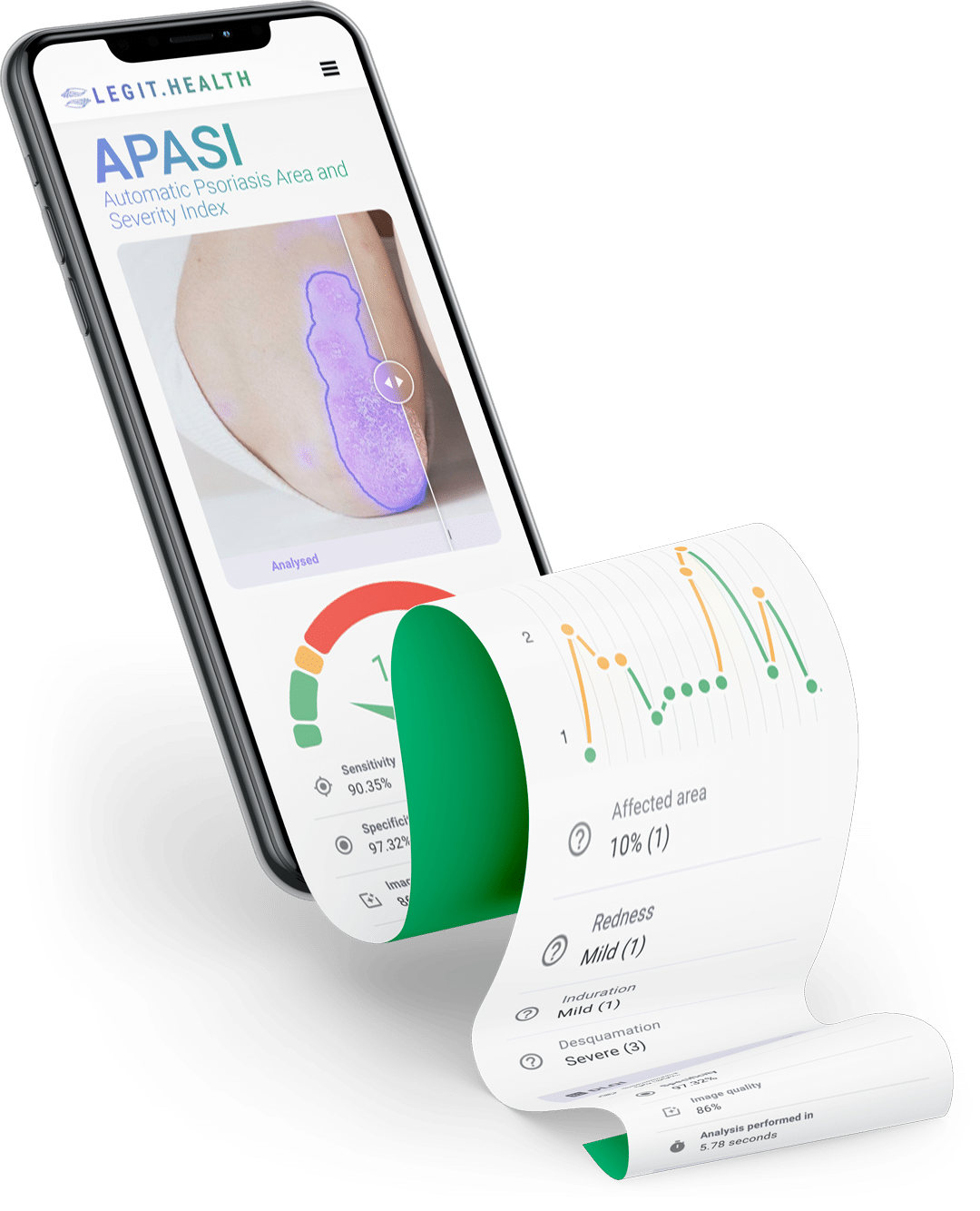
Automatic PASI severity scoring inside the consultation: an image becomes a reproducible number that travels with the patient.
Dermatology is not the easiest specialty to redesign, and no AI tool will fix workforce shortages on its own. But the three shifts named in the 10-Year Plan describe a pathway that, for skin disease, has been waiting for the data layer to catch up with the demand.
Why this matters now
Closing the gap will not come from one tool or one trust. It will come from the slow, unglamorous work of making the front door of dermatology better: better images, better data, better referrals, better follow-up. That is the work an AI-supported workflow is designed to do, and the case it has to make.
Quick recap
- 24% of UK GP consultations involve a skin complaint. 1
- ~13 million skin-related primary-care attendances every year in England. 2
- 17 weeks median wait for a first dermatology appointment in parts of England. 3
- 2-week-wait (2WW) pathway for suspected skin cancer is one of the largest urgent-referral cohorts in the system. 4
- AI-supported triage and severity scoring fits the NHS 10-Year Plan's three strategic shifts: hospital to community, sickness to prevention, analogue to digital.
Work with us
If you are a Primary Care Network (PCN) Clinical Director, an Integrated Care Board (ICB) digital lead, a GP with Extended Role (GPwER) in dermatology, a clinical director, a Chief Digital and Information Officer (CDIO), or a private hospital innovation lead, and you are working on dermatology pathway redesign, we would like to talk. Leave your details below and someone from our UK team will be in touch.