Dermatology deserts and digital frontiers: how Brazil is rebuilding the dermatology pathway




A clinician reviewing a case on the Legit.Health interface.
In a small town in the interior of the Northeast, a primary-care physician suspects melanoma in a 62-year-old patient. She writes a referral. The referral describes the lesion in words: there is no standardised photograph, no objective severity measurement, no structured baseline. The patient joins the queue. The queue moves at the speed of a continent: before telemedicine programmes began to compress it, the average wait for a dermatology appointment in the SUS reached 294 days. 1
Skin cancer does not wait 294 days.
This is the access deficit that defines Brazilian dermatology today, and it is a different deficit from the one other countries face. Brazil is a continental country with a dual health system, and the dermatology bottleneck is not one queue: it is two parallel queues, both under pressure, each for slightly different reasons. A clinically validated layer of artificial intelligence (AI) that covers the full spectrum of dermatology (skin cancer, chronic disease and longitudinal follow-up) and is certified by ANVISA, with CE marking and MHRA registration, is the missing piece in both queues.
World-class dermatology, unevenly distributed
Brazil has world-class dermatology. It is simply not evenly distributed.
According to the Brazilian Society of Dermatology (SBD), only 9.5% of Brazilian municipalities have at least one dermatologist, and about a third of the country's dermatologists practise only in the state of São Paulo. 2 Nationally, the ratio sits between 1 dermatologist for every 17,500 and 23,000 inhabitants, depending on the medical-demography survey; in remote regions of the North and Northeast that proportion is far lower, orders of magnitude below what the World Health Organization considers reasonable for a specialty whose demand spans cancer screening, chronic disease and primary care. 2
The result is a specialty that is everywhere in primary care, with virtually every family doctor handling dermatology day to day, but with specialist capacity concentrated in a handful of capitals. Geography becomes a clinical variable.
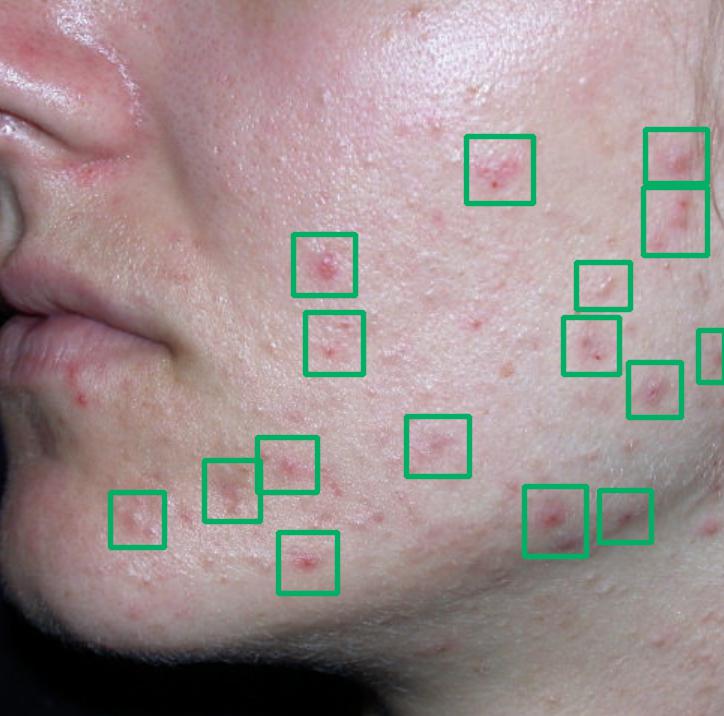
Diagnosis support across the full spectrum, from a chronic inflammatory disease to a benign vascular lesion, looks like this:
- Acne76.62%
- Malassezia folliculitis7.14%
- Seborrheic dermatitis1.79%
- Rosacea1.02%
- Eczematous dermatitis0.98%
- Acne
- Malassezia folliculitis
- Seborrheic dermatitis
- Rosacea
- Eczematous dermatitis
- Other
- Haemangioma85.87%
- Infantile papular acrodermatitis0.22%
- Zoster0.19%
- Epidermal nevus0.17%
- Angioma0.17%
- Haemangioma
- Infantile papular acrodermatitis
- Zoster
- Epidermal nevus
- Angioma
- Other

The mix matters. Skin cancer is the most urgent slice of dermatology, but it is far from the largest. The bulk of what primary care sees is chronic, inflammatory or infectious disease, and most of those cases could be resolved without a specialist slot.
Two parallel queues, one specialty under pressure
Brazil has the SUS (Sistema Único de Saúde, the public, universal health system) and a broad network of private health operators covering tens of millions of members. Dermatology is under pressure on both sides of that line, and the pressure looks different on each.
In the SUS, the bottleneck is volume meeting geography. A basic health unit in a small town has to triage dermatological complaints (benign nevi, suspected melanoma, eczema flares, chronic psoriasis follow-up, hidradenitis) in a single queue that may be served by a dermatologist hundreds of kilometres away. Telemedicine programmes such as the one in Rio Grande do Sul have shown that this queue can be cut by 79% when triage is structured at the source, but the gain depends on what reaches the specialist, not just on opening the channel. 1
In the private system, the pressure is different. Health operators are not short of dermatologists: they are short of a way to route teledermatology demand without sending every case to the specialist. A growing share of members is using teledermatology and integrated apps as the front door, and the operator faces two questions at once: which of these cases genuinely need a specialist, and how to make sure the ones that do arrive with enough information to be useful?
Both queues run into the same constraint underneath: the referral itself does not carry the data the next clinician needs.
Skin cancer is a counter, and it is running
Dermatology in Brazil is not only a chronic-disease story. Skin cancer is the most diagnosed tumour in the country: non-melanoma skin cancer is the most frequent cancer in Brazil, with about 263,000 new cases per year, more than 30% of all cancer diagnoses, according to INCA's 2026-2028 Estimate, which projects 781,000 new cancer cases per year in the country. 3 The longitudinal hospital data go further: skin cancer morbidity rose 86% above historical rates between 2012 and 2022, a trend driven by ageing, sun exposure and, critically, the interval between suspicion in primary care and confirmation by the specialist. 4
Every December, the Brazilian Society of Dermatology runs the Dezembro Laranja (Orange December) campaign for skin cancer prevention and early detection, with free screening drives at more than 100 sites across the country. It is a good seasonal moment to reinforce this conversation with the press and the Brazilian public.
Uneven geography weighs here because the patients with the longest distances to a dermatologist are precisely the patients whose lesions are least likely to arrive with an image on record at presentation. Distance becomes diagnostic delay. Diagnostic delay becomes a more advanced stage at presentation.
What an integrated remote-care flow would look like
The solution is not "more dermatologists". That is a 10-year answer to a 10-day problem. The solution is a layer that makes every referral, in either system, carry the same minimum dataset to the next clinician:
- A standardised image, captured the same way, regardless of the unit or the device.
- Diagnosis support: an AI-assisted read that flags clinical findings at the moment of triage and complements the clinician's judgement.
- An objective severity score, anchored in validated clinical scales (PASI, SCORAD, IHS4, UAS, SALT...) used in dermatology in Brazil today, rather than in the subjective impression of whoever is writing the referral.
- A structured longitudinal baseline, so that follow-up means measurement, not a fresh impression.

The patient starts the flow by sending a photo through the app they already use.
A 4-step flow, inside the operator's or hospital's own app
- The patient opens the hospital provider's or health plan's app and sends a photo of the lesion and a short structured history.
- A clinically validated AI returns a structured read of the image to the clinician: diagnosis support and an objective severity output.
- The clinician decides the most appropriate route: primary care (APS), specialist or teledermatology.
- The same record becomes the longitudinal baseline for any future review of that patient.
No second login, no parallel system: the data the next clinician needs travels with the patient.
Do you want to see the clinical AI technology in action?
A frontier moment for Brazilian digital health
Brazil is not lagging in digital health. On several dimensions, it is at the frontier. The Ministry of Health anchored its agenda in the Digital Health Strategy for Brazil 2020-2028 (ESD28), 5 runs one of the largest public teledermatology programmes in the world, is building national interoperability through the RNDS (National Health Data Network) on a Brazilian FHIR profile, 6 and is accelerating the SUS Digital Programme as the operational arm of that strategy.
On the regulatory side, ANVISA is actively reshaping the framework for software as a medical device. RDC 657/2022 aligned Brazil with the IMDRF SaMD framework, 7 and the revision of RDC 657, in public consultation by ANVISA since 2025, introduces a quality standard specific to AI-based SaMD, covering controllability, adaptability, robustness, transparency and intervention capability, alongside the Predetermined Change Control Plan (PCCP), a mechanism that allows AI products to be updated safely without reopening the registration at every iteration. 8 9
It is the same direction the FDA's AI/ML SaMD framework took, and Brazil is among the first emerging markets to formalise it.
The implication for operators, hospitals and primary-care programmes is concrete: the question is no longer whether a clinically validated AI fits the dermatology flow. The question is now which AI layer is regulated to operate inside that flow, on real clinical outcomes, with traceable clinical evidence and standards-based integration.
This is the bar a frontier digital-health stack has to clear:
- Regulated as a medical device, not as a wellness app: certified by ANVISA, with IFU available in Portuguese, CE marking in the European Union and registration with the MHRA in the United Kingdom.
- Clinically validated on outcomes that matter: diagnosis support and severity-scoring performance against dermatologist panels and validated clinical scales, not just retrospective accuracy on closed datasets.
- Built around the full spectrum of dermatology: skin cancer, chronic disease, general dermatology and longitudinal follow-up, because the frontier model of care is integrated, not fragmented by condition.
- Standards-based integration with the Brazilian electronic-health-record ecosystem, so that the AI output is structured data in the clinical record, not a screenshot.
- Engineered under ISO 13485 and ISO 27001, LGPD-compliant by design.
The next decade of dermatology in Brazil will not be won by the largest roster of specialists. It will be won by the operators, hospitals and public programmes that put the right layer of clinical-grade AI between the patient's photo and the specialist's queue, on rails the health record already understands.
For health operators and insurers
For a Brazilian health operator, the access deficit is also a utilisation and unit-cost problem: dermatology demand is growing, and the specialty is already among the five most sought-after on telemedicine platforms in Brazil. 10 Every unrouted referral ends up becoming a specialist appointment, and the operator has little visibility into what the specialist actually needed to see.
An AI-supported dermatology layer changes the unit of work the operator pays for.
Remote start by the patient
The member opens the app the operator already offers, the same app they use to book an appointment, request authorisation or talk to a teledermatology clinician, sends the photo of the lesion and answers a short structured history. No second app, no new login: the journey begins exactly where the member already is.
Routing by data, not by description
With a standardised image, diagnosis support and an objective severity score attached to the case, the operator's care-management team, or its teledermatology partner for health operators, can route by clinical signal: primary care, teledermatology, in-person specialist or urgent specialist.
Less leakage in the dermatology queue
Standardised triage at the source tends to reduce unnecessary specialist referrals, which compresses the chronic dermatology queue without having to expand specialist capacity.
An auditable clinical record
Every step, image, diagnosis support, severity score, triage decision and clinical decision, is structured and dated: exactly the kind of evidence the operator needs for clinical-governance review, audit and value-based contracts with the provider network.
The same pattern works for TPAs, self-insured corporate health programmes, telemedicine providers contracted by operators, and large hospital networks (Albert Einstein, Sírio-Libanês, Rede D'Or, Hapvida NotreDame Intermédica, Amil) that run their own digital front door. The integration target is the same: the platform the patient already uses.
Built for integration with the Brazilian electronic health record
A dermatology AI layer is only useful if the structured output it produces actually reaches the clinician, inside the system they already work in. That is a health-record integration problem, not an interface problem.
Legit.Health was designed to connect to the Brazilian electronic-health-record ecosystem: operators' care-management platforms, hospital records, primary-care information systems and teledermatology stacks. The integration is standards-based, and the AI output arrives as discrete clinical data in the patient record, rather than as a screenshot or PDF attachment. Data handling is LGPD-compliant end to end, with a legal basis, data minimisation, auditable access and data residency in national territory when required by the operator's policy.
In practice, the AI output becomes part of the longitudinal clinical record the operator and provider already keep, searchable, comparable across visits and reusable in follow-up, rather than an isolated screenshot inside a parallel system.
Where Legit.Health fits in the Brazilian market
Legit.Health is a regulated medical device, certified by ANVISA, with Instructions for Use (IFU) available in Portuguese, designed to operate exactly as the missing layer in the dermatology flow, covering the full spectrum of dermatology: skin cancer screening, diagnosis support, severity scoring in chronic disease and longitudinal follow-up.
It also carries CE marking, MHRA registration, ISO 13485 and ISO 27001 certifications, and was designed for LGPD-compliant integration with Brazilian electronic health records.
What this means in practice for a health operator, hospital network or primary-care programme in Brazil:
- The same standardised image, diagnosis support and objective severity score reach every clinician in the chain: primary-care physician, telemedicine physician, specialist.
- Referrals become routed by data, not by description, which takes pressure off the specialist queue without having to expand it.
- Chronic-disease follow-up becomes reproducible: the same lesion, measured the same way over time, regardless of which clinician is in front of the patient.
The uneven distribution of dermatologists will not change overnight. The 294-day queue will not disappear on its own. But the referral that enters the queue can stop being a paragraph of subjective text and become a structured clinical record, anchored in a standardised image, with diagnosis support and an objective severity score, which is exactly what every downstream queue, in either system, is waiting for.
Talk to the Brazil team
If you lead dermatology, primary care, telemedicine or a digital-health programme inside a health operator, a hospital network or a public-health initiative, and you want to see what an integrated, ANVISA-certified, LGPD-compliant dermatology AI layer would look like inside your specific flow, talk to the Legit.Health Brazil team.
About Legit.Health. Legit.Health is a regulated medical device for AI-supported dermatology, certified by ANVISA in Brazil, with CE marking in the European Union, registration with the MHRA in the United Kingdom, and ISO 13485 and ISO 27001 certifications. It was built for the full spectrum of dermatology (skin cancer screening, diagnosis support, severity scoring in chronic disease and longitudinal follow-up), and designed for LGPD-compliant integration with Brazilian electronic health records.